Prescription Copay Claim Form
Please read the information under the Prescription Copay Information tab prior to submitting for reimbursement. If you have any questions, please contact the SBF at (716) 881-5462.
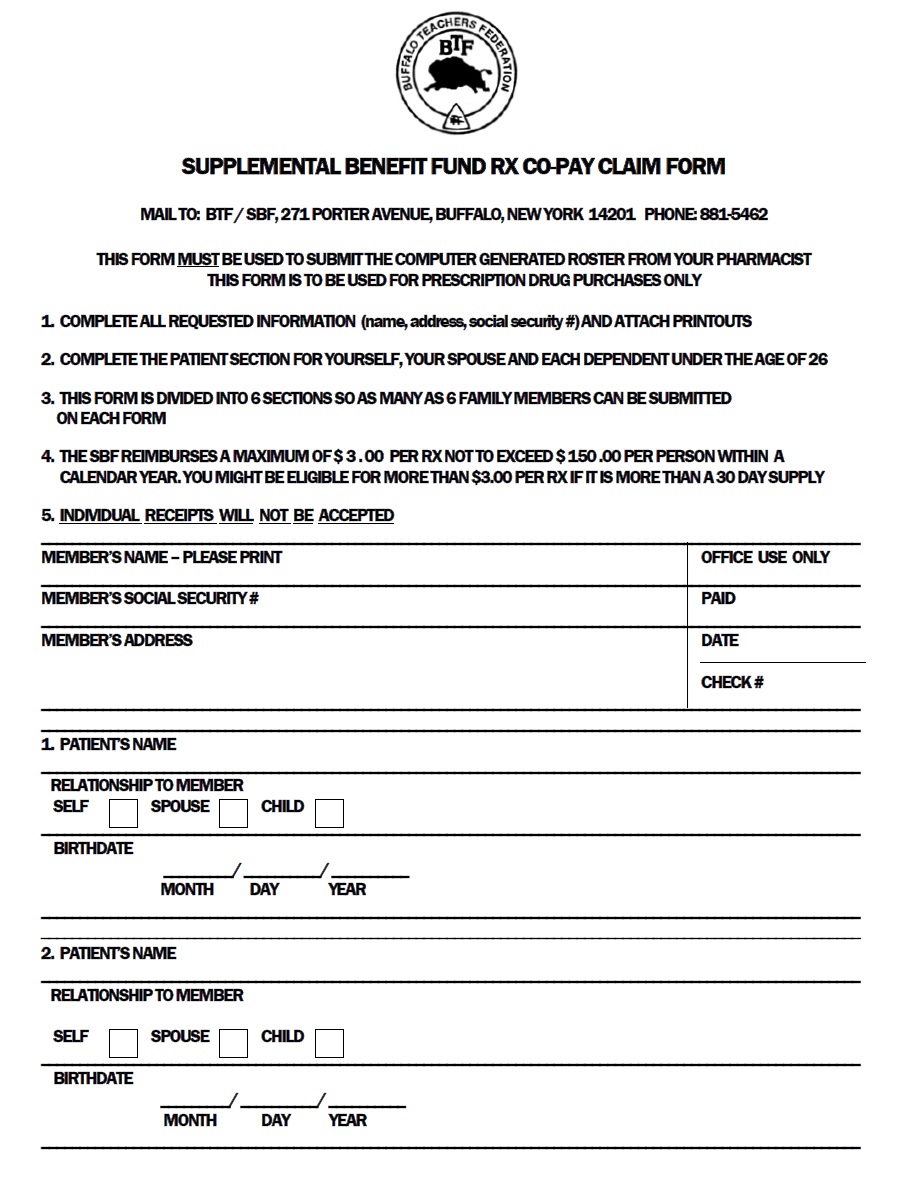
For more information regarding the SBF Prescription Copay Benefits, please see the Prescription Copay Information Section.